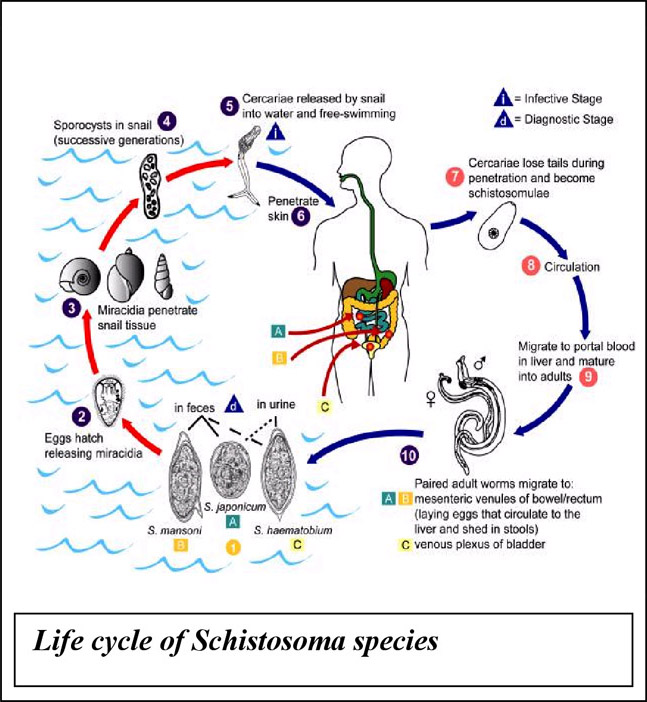
Diagnosis of Bilharzia
Laboratory diagnosis of Bilharzia is usually performed by microscopical detection of eggs in urine or stool or by immunological methods (antibody or antigen detection).
Microscopic diagnosis is the established gold standard for detecting and confirmation of an active Bilharzia infection. However, expert microscopic diagnosis are often not available, or may also delay the diagnosis of treatment in clinical suspected patients, or may be unreliable or absent in remote areas. The sensitivity of microscopic examinations also depends on the severity of the infection. In low grade infections, the sensitivity of one microscopic examination may be as low as 20%. In clinically suspected cases up to 5 urine specimens (collected over midday), and or 5 stool specimens for microscopic examinations are recommended to increase the sensitivity of the tests.
Due to immune modulation the infected host may show a separate IgG, IgM, IgA and IgE antibody response, or a combination of these isotypes. As much as 14% of patients may not respond with any antibody formation. Depending on the methodology used and the timing in the post infected host, the sensitivity of current antibody assays is not optimal (ranging from 65 to 86%). Some of the commonly used methodologies are based on detection of antibodies directed against the soluble egg antigen (SEA). Due to the retention of eggs and the constant secretion of SEA by the deposited eggs, antibodies may be elicited for an indefinite period after the primary infection, irrespective of successful treatment.
The urine-CCA cassette test is an antigen detecting test which is present in all Schistosoma species, including animal species. The major portion of CCA released by the adult live parasite is secreted in the urine. A positive CCA test result on randomly collected midstream urine indicates an active Bilharzia infection.